




















新車デリカD5 シャモニー納車させていただきました。
2017年12月26日
ご注文いただきました
新車のデリカD5 この季節の特別仕様車シャモニー
クリーンディーゼルを納車させていただきました。


なんと納車日はクリスマス

合わせた訳では無いんですけどね。
24日にボディーにポリマーコーティングを施工したのが最後の作業で
お渡しが25日となりました

ポリマーコーティング施工中
あ、両サイドに貼ってある
10周年記念シャモニーステッカーはご要望で剥がしました。
ナビとバックカメラの取り付け作業の様子
バラバラです

ステアリングリモコン対応ナビなので、操作ラクラクです

デリカはワイドナビが入るので
パナソニックの新しい7型ワイドRE04WDをインストール
取付キットを探すのが大変でした・・・(´・ω・`)
灯台下暗しとはこの事。
純正取り付け金具でOKだとは・・・(笑)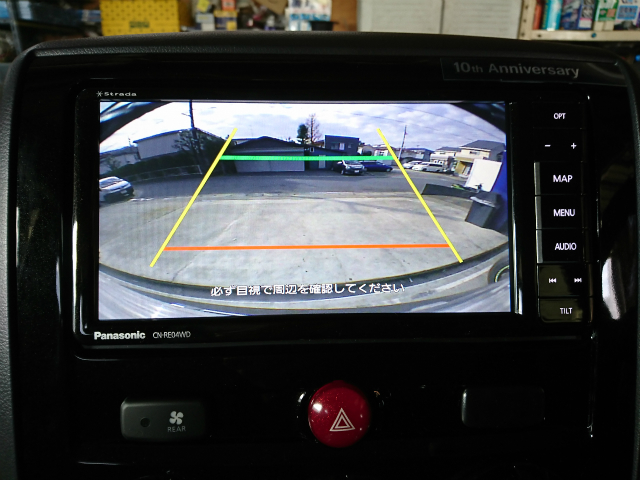
バックカメラもリアガーニッシュ内に綺麗に収まりいい感じです♪
ピッピッッ の純正ホーンだとアレなので、
の純正ホーンだとアレなので、
アルファホーンに変更
来年にはモデルチェンジなデリカD5ですが、
お客さまのご要望どおりの
ステキな最終モデル シャモニーに仕上がりました
ご購入からカスタマイズのお手伝いまで出来て僕も楽しかったです
いつもありがとうございます。
レストガレージ阿部